BRUNNSTORM'S APPROACH
INTRODUCTION
It was developed by Signe Brunnstorm, a Swadish American physiotherapist. It is a neurophysiological treatment approach, that has been conceptualised from two important theories of motor control namely- a)Reflex Control Theory b)Herarchial Control theory
a) Reflex Control Theory:- In this theory, reflexes are the building blocks to complex motor control and movement.It says that afferent sensory inputs are necessary prerequisite for efferent motor output. We can understand this by an example:- In acute hemiplegic patients, at day 1 or day 2, there is no movement or flaccidity, there is no reflex activity or no movement. In this situation, brunnstorm states that we should first utilise techniques which will facilitate and use reflex to regain motor control in hemiplegic patients.
b)Hierarchial Control Theory:- It states that CNS is organised in hierarchy levels to control motor functions of the body.
PATHOPHYSIOLOGY
*In normal individual, the motor response of the mid brain, brainstem and spinal cord are controlled by the higher centers (cortex).
*Certain motor behaviours at subconscious and reflexive levels are processed at spinal cord, brainstem and mid-brain level.

*Stroke appears to result in development in reverse, recovery of voluntary movement post stroke proceeds in sequence --
- first the therapist should try to facilitate reflexive movements that are mediated by brainstem and spinal cord.
-followed by more complex movements that are mediated by mid-brain. (flexor synergy, extensor synergy)
-once the patients gain control over these synergies, then brunnstorm recommends now we should progress towards producing more complex motor behaviour which are mediated by higher centers (cortex).
*Proprioceptive and exteroceptive stimulus can be used to evoke desired motor or toner changes
* Progress the patient from lower to higher motor center.
BASIC LIMB SYNERGIES
Limb synergies are intensive of associative reaction. They may occur either reflexively or as early stage of voluntary control when spasticity is present.
When the patient initiates movement at one joint, all the muscles that are linked in synergy with that movement automatically contract causing stereotypyped movement pattern.
Hemiplegic patient cannot perform isolated movements when they are bound by any synergy, example:- a hemiplegic patient wants to flex his elbow, then he won't be able to do it without producing scapular retraction and elevation and shoulder abduction. So everytime he want to flex the elbow, he will be accompanied by activation of rest of muscle of this synergy.
-: UPPER-LIMB SYNERGY:-
-:FLEXOR SYNERGY
-: EXTENSOR SYNERGY
-: MIXED SYNERGY
1. FLEXOR SYNERGY

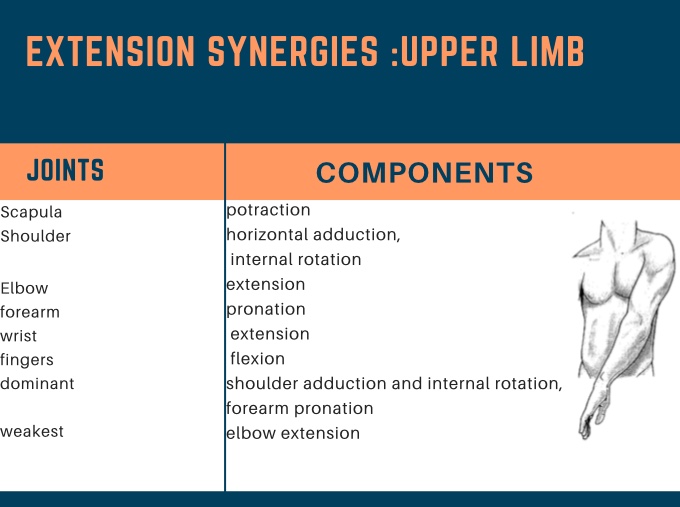
2. EXTENSOR SYNERGY
3. MIXED SYNERGY

-: LOWER LIMB SYNERGY
-:FLEXION SYNERGY
-:EXTENSOR SYNERGY
-: MIXED SYNERGY
1.FLEXOR SYNERGY

2. EXTENSOR SYNERGY

3. MIXED SYNERGY





So lot to occur over your amazing blog. Your blog procures me a fantastic transaction of enjoyable.. Salubrious lot beside the scene. Physical Therapy
ReplyDelete