INTRODUCTION:- Reflexes are the involuntary and instantaneous movement in response of a stimulus. It is an automatic response to a stimulus that does not need conscious thought on an impulse as it occurs through a reflex arc.
REFLEX ARC:- It contains only two neurons, a sensory and a motor neuron. Sensory neuron receive the stimulus from the receptor and transport it to spinal cord. From here, information is carried to the muscle by efferent or motor neuron to get the response.
👉 Abdominal reflex:- Technique- Abdominal wall is lightly stroke from without inwards stimulating each of the quadrants of abdomen. Response- The muscle in quadrant stimulated and the umbilicus moves in that direction.
👉 Planter reflex:- Technique- The patient is positioned such that the knee is fixed and thigh is slightly externally rotated. Examiner fixes the ankle joint by rotating it and then outer aspect of sole is shocked with a blunt point (key). The stroke is directed forwards and then it curves inwards along the MTP joints from the little to big toe. Response- Normally the great toe will flex at the MTP joint accompanied by flexion of other toes.
👉 Corneal reflex:- Technique- The corneal edge is touched by the whisk of cotton with the patient looking in opposite direction.
Response- Brisk closure of the eye
DEEP REFLEXES-
👉 Jaw jerk:- Technique The patient is asked to keep his mouth partly open with his mandible hanging loosely. Finger is placed over the chin and tap the hammer on the finger.
Response- slight of elevation of the mandible.
👉 Biceps jerk:- Technique- The upper limb is partially flexes at the elbow. Press the forefinger gently on the biceps tendon in the cubital fossa and then strike the finger with knee hammer.
Response- Flexion of elbow and visible contraction of biceps tendon.
👉 Supination jerk:- Technique- The upper limb is partially flexed at elbow in mid-prone position. Strike the lower end of radius about 5cm above the wrist,
Response- Contraction of brachioradialis and flexion of elbow.
👉 Knee jerk:- The knees are partially flexed and rested on the examiners forearm. The quadricep tendon is the striked with a knee hammer.
👉 Ankle jerk:- Technique- The patients leg is extremely rotated and flexed at the knee. The patients forefoot is gently dorsiflexed. The Achilles tendon is striked with a knee hammer.
Response- Planter flexion of foot and visible contraction of gastroecnemius muscles.
* It is unusual for a specific lung function test to diagnose a disease. A series of tests may be done to diagnose the lung disorder to one of several categories and when other features such as history, physical examination, radiology and pathology are added, a complete/possible diagnosis is considered.
AIMS OF PFT
💧 to define more clearly the type of functional disorder.
💧 to measure the progression or regression of the disorder.
💧 to decide the feasibility of thoracic surgery
💧to assess the degree of respiratory failure.
CLASSIFICATION OF PULMONARY DISEASE ACCORDING TO THE PFT
The PFT provides the basic classification of pulmonary disease into three major pathological categories:
i) OBSTRUCTIVE LUNG DISEASE:- When there is any obstruction in the airways. It is characterised by decreased forced expiration.
ii) RESTRICTIVE LUNG DISEASE:- It is characterised by decreased lung volumes.
iii) COMBINED LUNG DISEASE:- It involves both i.e. decreased inflow and lung volumes.
PARAMETERS OF PFT
i) measurement of lung size.
ii) measurement of ease of flowing of air in and out of the lungs
iii) measurement of efficiency of gaseous exchange process.
CATEGORIES OF PFT
i) Ventilatory Function Test
ii) Arterial Blood Gas analysis/ Test for gaseous exchange
iii) Exercise Tolerance Test
1. VENTILATORY FUNCTION TEST
A spirometer is used for testing the ventilatory of an individual. The patient is asked to breathe in as far as he/she can and breathe out maximally as possible. This volume of air is called the vital capacity. The vital capacity when measured by the spirometer in which the deepest breathe in is followed by forced breathe out is called Forced Vital Capacity.
The maesure of vital capacity and FVC gives an indication of the ventilatory capacity of the lungs.
In normal individual the VC and FVC are approximately equal. But in case of COPD, the compression of the airways during forced expiration causes an earlier closure of airway
in COPD, FVC<VC
The volume of air that can be breathe out during a forceful expiration in 1st second is called FEV1 (Forced Expiratory Volume in 1st second). Normally, the FEV1 is 70% of FVC. In case of COPD, expiration is prolonged and so that ratio of FEV1/FVC is decreased. In restricted lung disease, there is a restriction in lung expansion but no effect on the airways. So, FEV1 and FVC are reduced but their ratio remains normal.
Spirometer
2. ARTERIAL BLOOD GAS ANALYSIS
OR
TEST OF GAS EXCHANGE
For efficient respiratory gas exchange, the major process of lung ventilation, diffusion across the alveolar-capillary membrane and lung perfusion should be intact. We check it by ABG analysis (Arterial Blood Gas analysis).
ABG analysis is an essential part of diagnosis and managing of patient oxygenation status and acid-base balance. The pH is the measurement of the "acidity" and "alkalinity" of blood. It is inversely proportional to the number of H+ ions in the blood. It means more the H+ ions, less will be the pH and vice versa. The pH is measured on the scale from 1-14.
The normal blood pH is 7.35-7.45, in order for normal metabolism to take place, the body must maintain this narrow range all time. Below 7.35, the blood is acidic and above 7.45, the blood is basic or alkaline.
*significant changes in blood above pH 7.8 or below 6.8 will interfere with cellular functioning and if it is uncorrected it will lead to death.*
RESPIRATORY BUFFERRESPONSE:- A normal biproduct of cellular metabolism is CO₂. CO₂ is carried in the blood to lungs where excess CO₂ combines with water to form carbonic acid H₂CO₃. The blood pH will change according to level of carbonic acid present. This triggers the lung either to increase or decrease the rate and depth of the ventilation until the appropriate amount of CO₂ has been establish. Activation of lungs to compensate for balance starts within 1-3 minutes.
RENAL BUFFER RESPONSE:- In an effort to maintain the pH of blood within its normal range, kidney excretes or retain bicarbonate. As the blood pH decreases the kidney will compensate it by retaining bicarbonate and as the pH rises the kidney excretes bicarbonate ions through the urine. This provides an excellent means of regulating acid-base balance. The system may take from hours to days to correct the imbalance.
* When respiratory system and renal system are working together they are able to keep blood pH balanced.
ACID-BASE DISORDERS
💧 Respiratory acidosis
💧 Respiratory alkalosis
💧 Metabolic acidosis
💧 Metabolic alkalosis
RESPIRATORY ACIDOSIS
It is defined as a pH less than 7.35 with PaCO₂ greater than 45mmHg. Acidosis is caused by an accumulation of CO₂ which combines with water in the body to produce carbonic acid thus lowering the pH of blood.
RESPIRATORY ALKALOSIS
It is defined as a pH > 7.45 with PaCO₂ < 35mmHg. Any condition that causes hyperventilation can result in respiratory alkalosis.
METABOLIC ACIDOSIS
It is defined as a bicarbonate level < 22meq/l with the pH < 7.35.
METABOLIC ALKALOSIS
It is defined as the bicarbonate level > 26meq/l with pH > 7.45.
3. EXERCISE TOLERENCE TEST
Spirometry alone cannot predict about how much a person can walk.Nor the asking the patient is reliable. Hence ETT can give an accurate assessment. As walking can affect our cardiopulmonary system, so this test can assess these functions.
So, ETT is used to assess the patients capacity to tolerating breathing intensity of exercise while ECG, B.P., Heart rate and symptoms re monitored for the evidence of myocardial ischemia, abnormal electrical conduction or other abnormal sign and symptoms of congestion.
TYPES OF TESTS:- Treadmill test, six-minute walk test, cycle ergometer, upper limb ergometer, stairs climbing.
PROCEDURE:- Before exercising, the patient is hooked up to EKG machine. The patient is required to exercise at progressively greater impedence of work while increase of the speed and grade of treadmill or increase the speed and resistence to padelling the extremity on bicycle ergometer.
Traumatic Brain Injury (TBI) is defined as "an alteration in brain function, any brain pathology, caused by an external force.
Because of the multiple body systems affected by a brain injury and its secondary impairment, a physiotherapist must be proficient in examination procedures and intervention techniques.
Because of the wide variety of presenting impairments, TBI requires a strong interdisciplinary team for its maintenence. Physiotherapist is an important member of this team.
It is important to remember that The patient is the central member of the team.
ASSESSMENT SCALES
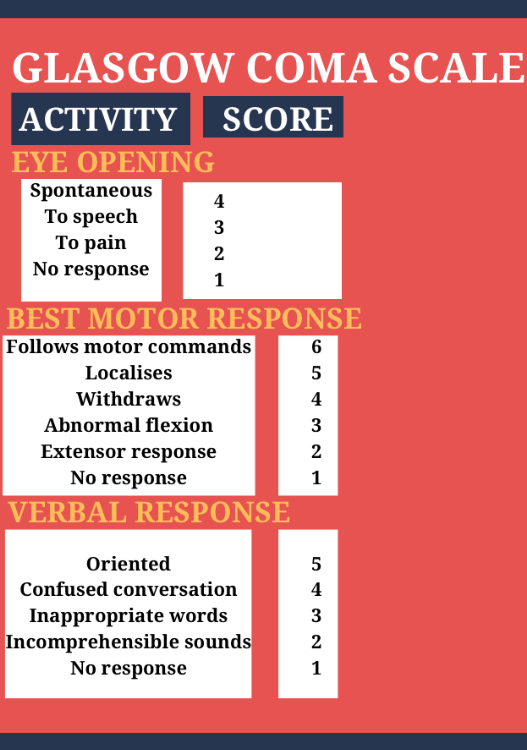
1. GLASGOW COMA SCALE:-
This scale was developed by Teasdale and Jennett. It measures the level of consciousness andclassify the severity of injury.
It is comprised of three response scores:-
a) MOTOR RESPONSE
b) VERBAL RESPONSE
c) EYE OPENING
Scores of 8 or less are classified as severe and having coma, scores between "9-12" are defined as moderate, and scores of "13-15" are classified as mild brain injury.
2. RANCHOS LOS AMIGOS LEVEL OF COGNITIVE FUNCTIONING
This is a descriptive scale that outlines a predictable sequence of cognitive and behavioural recovery seen in TBI.
ROLE OF PHYSIOTHERAPIST
The following section will breakdown physical therapy management according to Ranchos Los Amigos LOCF scale. However, the physical return does not mirror the cognitive and behavioural recovery i.e. just because the patient is moving from grade 4-grade 5 does not mean that they will show similar gain in physical function. Among the 2 grade IV patients, one may remain confused to wheel chair while the other ambulate independently.
RANCHOS LOS AMIGOS LEVEL I, II, III (DECREASED OR LOW RESPONSE LEVELS)
The first step in the beginning of an examination of a patient at these stages of recovery is to conduct a comprehensive chart review because of strong likelihood of various precautions and complications seen in this patient population.
By doing a complete chart review the therapist is able to form a picture of the patient in his mind.
Observe the patient's:-
a) posture
b) eyes- open/closed
c) track of auditory/visual stimulation
d) vocalise
e) any active movement- purposeful/non-purposeful
f) reaction to painful stimuli
g) change of vital signs.
a) Improving Arousal through Sensory Stimulation:-
When performing PROM the therapist should talk to the patient. The therapist should explain and demonstrate treatment techniques to the patient. This provides tactile, auditory, painful, proprioceptive and visual sensation. The therapist should engage the patient by asking him or her to attempt to move the limb while performing PROM.
Secondary stimulation is provided in a discrete manner. Example:- photograph of family memebers, music, or food tastes.
MODES
AUDITORY STIMULATION:- Normal conversational tone to explain what's to be done.
-discussion of topics that have meaning (logical)
- intermittent use of radio/television but constant background voice is desirable.
VISUAL STIMULATION:- provided by the use of familiar objects.
- it is important to stimulate all areas of visual field to compensate for visual field defects
OLFACTORY STIMULATION:- provided by placing scents under the patients nose for 15-20 seconds.
- Patient with traecheoctomy are not likely likely to respond because they do not breath through nose.
GUSTATORY STIMULATION:- application of cotton swab dipped in flavoured solution to lip and gums
- A therapist skilled in dysphazia management should be involved in this treatment due to increased risk of aspiration.
b) Preventing secondary complications
Because of patients inability to move in these stages they are more susceptible to various secondary impairment.
- Proper positioning both in bed and in wheelchair as it prevents skin breakdown, contractures and assist in pulmonary hygiene.
- In bed head to be kept in neutral position to prevent neck contractures and lessen the effect of tonic reflexes.
- Turning helps to prevent skin breakdown and pneumonia so should be turned every 2 hours.
- Proper wheel chair positioning is important. Splints can be used to promote positioning.
- P.D, percussion and vibration are used co-operatively by respiratory care. However, percussion should be referred in case of ICP.
- Passive ROM prevents contractures and DVT, may decrease hypertonicity and provides sensory stimulation.
As soon as the patient is medically stable, the patient should be transferred to a sitting position and out of the bed to the wheel chair. The patient should have adequate head and neck control to maintain and balance upright posture.
Use of tilt table is most advantageous because it allows early weight bearing through lower limb while upright positioning improves overall level of alertness.
The therapist helps the patient to interact with the environment as this aids the patient in learning by guiding the patient body in performance of functional task.
e) Patient and family education
It is important to educate the family about the stages of recovery. The therapist tries to involve family members in treatment session and teach them to perform PROM and sensory stimulation. They should be trained for proper positioning so that they can effectively perform them when therapist is not there.
RANCHOS LOS AMIGOS LEVEL IV
At this the patient is confused, so the patient should be seen by the person at the same time and place everyday.
Assume a calm and focussed affect to reduce the aggregation of patient to make them feel safe.
Give many options and safe choices.This will let the patient feel that he/she may have some control over the situation.
The patient cannot be expected to see other's point of view, he or she will be able to think only of themselves.
RANCHOS LOS AMIGOS LEVEL V & VI
The chief goal at this stage is to maximise functional mobility skills
Treatment sessions should be planned to maximise patients motor learning capabilities.
A memory book can be used, where daily schedule is placed in a notebook.
A swiss ball can be used to improve balance, modify tone and improve trunk control.
RANCHOS LOS AMIGOS LEVEL VII & VIII
The major goal is to assist the patient in integrating cognitive, physical and emotional skills that are necessary for function in the real world.
Involve the patient in decision making.
Group therapy can be given.
Talk to survivors of brain injury or a family member who has gone through same difficulties is of great benefit.
Physiotherapy is a medical science which is gaining rapid popularity. In this, there is no use of lots of injections, medicine or any surgery to treat the patient while it uses manual techniques.
Physiotherapy may be considered as a paramedical science but it is highly advanced. Researches are taking place in physiotherapy and new techniques are developed everyday.
Some people think that PT treats only those patient who have muscular or skeletal problems but this is not true. PT is necessary in other problems also like cardiovascular, geriatric, pediatric, antenatal, postnatal, and many more such conditions.
Basically, PT uses several exercises, manipulation, mobilisation, traction, heat and cold therapy, paraffin wax bath, electrotherapeutic modalities like TENS, U.S., LASER, IFT, electrical stimulation and many other techniques.
With the help of proper exercises, massages, manipulation, or other physiotherapy technique, a patients conditions can improve significantly.
Patient with TBI present with abnormalities of muscle tone. Mostly manifested as increased tone, hypertonia or spasticity.
Stretching and strengthening exercise with adjuctive modalities and functional retraining.
PROM and selective strengthening of antagonist muscles.
Proper positioning, maintaining head and neck in neutral position to minimize the effect of primitive reflexes.
Splints and serial casting can also assist in decreasing hypertonicity. These devices maintain a constant stretch and thereby increase the ROM and decrease tone. Serial casting prevents biceps and planter flexion contractures. Positioning splints will temporarily decrease tone, wrist and hand splints are effective. They prevent prolong shortening of muscles.
Neurostimulation can cause inhibition of abnormally high tone. The stimulation can be applied either to agonist/antagonist weight wearing on the affected limb, rhythmic rotation and aquatic therapy.
Botox and Phenol nerve blockers are synergistic anti-spasticity intervention. Botox paralyses the muscles to which it is administrated and prevents pre-synaptic nerve from releasing acetylcholine into the synaptic cleft such that hyperactive CNS cannot effect muscle contraction.
Phenol demyelinates nerves in lower concentration and denatures axonal protein at higher concentration.
Botox can best be administrated in highly innervated site such as intrinsic muscle of hand, paraspinals, pectoralis major, etc.
Medications prescribed to treat spasticity includes baclofen, tizanidine, clonidine, diazepam and dantrolene.
Surgical interventions include orthopaedic tenotomies as well as neurological ablative non-destructive procedures. Rhizotomy also performed to treat severe spasticity by baclofen pump implantation in the abdominal wall.
Concave-Convex rule was given by Freddy Kaltenborn. It is basically used to determine the appropriate direction of translational glide in order to determine which part of the joint capsule should be mobilised.
The direction in which sliding occurs depends on whether the moving surface is concave or convex.
CONCAVE = Hollowed or rounded inward
CONVEX = Curved or rounded outward
If the moving part is concave then, the slide/ glide is in SAME direction as the angular movement of the bone.
EXAMPLES:-
1. TIBIOFEMORAL JOINT:- The moving part is tibia (concave) on the femoral condyles (convex) so, if anyone is flexing his knee, the tibia moves posteriorly same with the movement.
If the moving part is convex then, the slide/glide is in OPPOSITE direction as the angular movement of the bone.
EXAMPLE
1. GLENOHUMERAL JOINT:- In this joint, the moving part is convex humeral head which moves on the glenoid fossa (concave), So according to concave-convex rule, if anyone does abduction then the humeral head will move in opposite direction that is inferiorly to the movement of the arm.
2. HIP JOINT:- In this joint, the moving part is convex femoral head which moves on the acetabulum (concave), So according to concave-convex rule, if anyone does flexion or abduction, the movement occurs in upward direction but the motion of moving bone will be inferior.
The rotator cuff is a group of muscles that surround the shoulder joint. These rotator cuff muscles keep the head of the humerus in the glenoid cavity of the scapula that means these muscles are the stabilizers of the glenohumeral joint.
There are 4 muscles in rotator cuff:-
👉 supraspinatus
👉 infraspinatus
👉 teres minor
👉 subscapularis
CAUSES OF ROTATOR CUFF INJURIES
RC injuries are common injuries that can occur at any age. In younger group, overhead activity performed in repetitions can lead to trauma on muscles, as seen in throwers, badminton players, bowlers, painters, cleaners, etc. With increase in age, the RC injuries may be due to muscle degeneration, impingement and tearing.
CLINICAL FEATURES OF RC INJURIES
Clinical features will depend upon the size of tear. The rotator cuff tear can be divided into grades:-
👉 grade 1- a tear of less than 1cm
👉 grade 2- a tear of 1-3cm
👉 grade 3- a tear of 3- 5cm.
👉 grade 4- complete tear of more than 5cm
Symptoms will depend upon the grades and location of tear. Normally, tear are located in 3 region:-
👉 Superior region
👉 supero-posterior region
👉 supero-anterior region
Pain is the chief complaint of the patient with RC tear.
Supero-anterior location of tear will have pain in bicipital groove area. Supero-posterior location of tear will have pain on the posterior region of humerus and will also have subscapularis muscle affected. Such patient will completely unable to perform internal rotation.
Restriction of movement will also vary with above grades and location. Grade 1 and grade 2 will have difficulty in performing overhead activity and repeated external rotation. Grade 3 and 4 will show sign of superior instability.
Strength of rotator cuff muscles will be diminished not beyond 2+ although scapular stabilisers will be strong.
Functional inability will be noted in performing activities like combing, wearing clothes, reaching overhead objects, etc.
DIAGNOSTIC TEST OF RC PATHOLOGY
Hawkins Kennedy test
Neer's Impingement Test
Empty Can test
Painful arc test
MANAGEMENT
Grade 1 and Grade 2 tear can be treated conservatively, like pain management by TENS, IFT, U.S. LASER, etc
If conservative treatment is not giving any result then we have to undergo surgical treatment and same protocol is followed for grade 3 and grade 4.
GOALS OF TREATMENT
👉 to maintain the integrity of rotator cuff, do not overuse the healing tissue.
👉 to reestablish dynamic humeral head control which means maintenence of scapula rythm and avoiding shoulder shrugging movement
👉 to reestablish muscular balance.
👉 to improve the R.O.M. of shoulder especially in external and internal rotation and elevation
👉 to restore the patients functional ability.
PROTOCOL FOR THE MANAGEMENT OF SURGICAL CORRECTION
It was given by Cohen and Romeo.
Immediate post operative, Iceing to the/ localised cryotherapy around the site of incision, no R.O.M exercises at shoulder and full R.O.M. at elbow and hand.
Initiation of R.O.M. at shoulder will depend upon size of tear. If the tear is 1cm, then the exercise should be started from 15 days, medium tear (1-3)cm- no R.O.M. for 3 weeks. Large tear (3-5)cm - no R.O.M. for 5 weeks. Massive tear - sling is applied for 6 weeks.
Perform isometrics of all shoulder muscles to prevent muscular weakness due to immobilisation.
If R.O.M. is initiated in shoulder, it is done passively by the therapist upto a limit of flexion 120 degree, abduction not beyond 90-100 degrees and rotation not 30 degrees.
No strengthening of muscle in this range is done.
6-8 weeks, strengthening of muscles in the available range can be started and continued for further 2 weeks using theraband.
10-12 weeks, increase the R.O.M. of shoulder performing active assisted exercises using WAND and PULLEY exercises upto the limit of forward flexion upto150-160 degree, abduction upto 120 degrees and rotation upto 60 degrees.
12-14 weeks, begin with strengthening exercises of shoulder using weight cups or manual resistence.
Upto 16 weeks, the patient achieves full R.O.M. full strengthening and full functional ability.
After 4 months, the patient is put on a home exercise programme which requires performence of capsular stretches in anterior, posterior, and inferior direction maintaining of shoulder strength by performing resisted exercises of shoulder using weight, cuff, medicinal balls.
In case of instability, due to injury to surrounding ligaments and labrum with R.C. muscle tear, the protocol of management will be the same except the duration of rehabilitation will increase.