INTRODUCTION
Traumatic Brain Injury (TBI) is defined as "an alteration in brain function, any brain pathology, caused by an external force.
Because of the multiple body systems affected by a brain injury and its secondary impairment, a physiotherapist must be proficient in examination procedures and intervention techniques.
Because of the wide variety of presenting impairments, TBI requires a strong interdisciplinary team for its maintenence. Physiotherapist is an important member of this team.
It is important to remember that The patient is the central member of the team.
ASSESSMENT SCALES
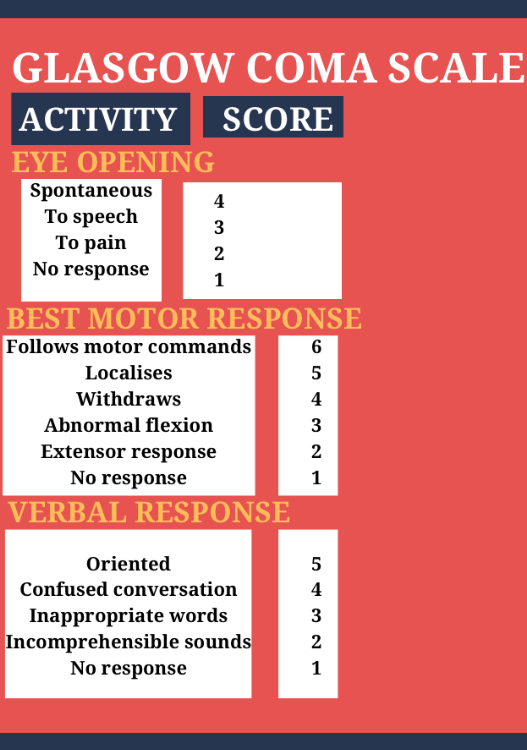
1. GLASGOW COMA SCALE:-
This scale was developed by Teasdale and Jennett. It measures the level of consciousness and classify the severity of injury.
It is comprised of three response scores:-
a) MOTOR RESPONSE
b) VERBAL RESPONSE
c) EYE OPENING
Scores of 8 or less are classified as severe and having coma, scores between "9-12" are defined as moderate, and scores of "13-15" are classified as mild brain injury.
2. RANCHOS LOS AMIGOS LEVEL OF COGNITIVE FUNCTIONING
This is a descriptive scale that outlines a predictable sequence of cognitive and behavioural recovery seen in TBI.



ROLE OF PHYSIOTHERAPIST
The following section will breakdown physical therapy management according to Ranchos Los Amigos LOCF scale. However, the physical return does not mirror the cognitive and behavioural recovery i.e. just because the patient is moving from grade 4-grade 5 does not mean that they will show similar gain in physical function. Among the 2 grade IV patients, one may remain confused to wheel chair while the other ambulate independently.
RANCHOS LOS AMIGOS LEVEL I, II, III (DECREASED OR LOW RESPONSE LEVELS)
The first step in the beginning of an examination of a patient at these stages of recovery is to conduct a comprehensive chart review because of strong likelihood of various precautions and complications seen in this patient population.
By doing a complete chart review the therapist is able to form a picture of the patient in his mind.
Observe the patient's:-
a) posture
b) eyes- open/closed
c) track of auditory/visual stimulation
d) vocalise
e) any active movement- purposeful/non-purposeful
f) reaction to painful stimuli
g) change of vital signs.
a) Improving Arousal through Sensory Stimulation:-
When performing PROM the therapist should talk to the patient. The therapist should explain and demonstrate treatment techniques to the patient. This provides tactile, auditory, painful, proprioceptive and visual sensation. The therapist should engage the patient by asking him or her to attempt to move the limb while performing PROM.
Secondary stimulation is provided in a discrete manner. Example:- photograph of family memebers, music, or food tastes.
MODES
AUDITORY STIMULATION:- Normal conversational tone to explain what's to be done.
-discussion of topics that have meaning (logical)
- intermittent use of radio/television but constant background voice is desirable.
VISUAL STIMULATION:- provided by the use of familiar objects.
- it is important to stimulate all areas of visual field to compensate for visual field defects
OLFACTORY STIMULATION:- provided by placing scents under the patients nose for 15-20 seconds.
- Patient with traecheoctomy are not likely likely to respond because they do not breath through nose.
GUSTATORY STIMULATION:- application of cotton swab dipped in flavoured solution to lip and gums
- A therapist skilled in dysphazia management should be involved in this treatment due to increased risk of aspiration.
b) Preventing secondary complications
Because of patients inability to move in these stages they are more susceptible to various secondary impairment.
- Proper positioning both in bed and in wheelchair as it prevents skin breakdown, contractures and assist in pulmonary hygiene.
- In bed head to be kept in neutral position to prevent neck contractures and lessen the effect of tonic reflexes.
- Turning helps to prevent skin breakdown and pneumonia so should be turned every 2 hours.
- Proper wheel chair positioning is important. Splints can be used to promote positioning.
- P.D, percussion and vibration are used co-operatively by respiratory care. However, percussion should be referred in case of ICP.
- Passive ROM prevents contractures and DVT, may decrease hypertonicity and provides sensory stimulation.
c) Spasticity management
d) Earlymobilisation
As soon as the patient is medically stable, the patient should be transferred to a sitting position and out of the bed to the wheel chair. The patient should have adequate head and neck control to maintain and balance upright posture.
Use of tilt table is most advantageous because it allows early weight bearing through lower limb while upright positioning improves overall level of alertness.
The therapist helps the patient to interact with the environment as this aids the patient in learning by guiding the patient body in performance of functional task.
e) Patient and family education
It is important to educate the family about the stages of recovery. The therapist tries to involve family members in treatment session and teach them to perform PROM and sensory stimulation. They should be trained for proper positioning so that they can effectively perform them when therapist is not there.
RANCHOS LOS AMIGOS LEVEL IV
At this the patient is confused, so the patient should be seen by the person at the same time and place everyday.
Assume a calm and focussed affect to reduce the aggregation of patient to make them feel safe.
Give many options and safe choices.This will let the patient feel that he/she may have some control over the situation.
The patient cannot be expected to see other's point of view, he or she will be able to think only of themselves.
RANCHOS LOS AMIGOS LEVEL V & VI
The chief goal at this stage is to maximise functional mobility skills
Treatment sessions should be planned to maximise patients motor learning capabilities.
A memory book can be used, where daily schedule is placed in a notebook.
A swiss ball can be used to improve balance, modify tone and improve trunk control.
RANCHOS LOS AMIGOS LEVEL VII & VIII
The major goal is to assist the patient in integrating cognitive, physical and emotional skills that are necessary for function in the real world.
Involve the patient in decision making.
Group therapy can be given.
Talk to survivors of brain injury or a family member who has gone through same difficulties is of great benefit.




No comments:
Post a Comment